

Introduction:
On March 11, 2020, the World Health Organization (WHO) declared SARS-CoV-19 a pandemic with about 114 countries affected. Many studies and metanalyses have investigated the risk factors associated with poor outcomes from COVID-19 infection. Different clinical as well as laboratory parameters have been shown to correlate with disease severity, including age, male gender, smoking history, presence of one or more co-morbidities, heart disease, hypertension, diabetes, obesity, and chronic lung disease.
Among these risk factors, several studies suggest that a decreased platelet count is associated with more severe disease course. A lower platelets count was also observed to be associated with a poor prognosis. On the contrary, not all reports seem to show the same association.
Objective:
Our study is aimed at investigating the prognostic impact of the platelet count in patients admitted with COVID-19 infection and understanding its association with disease severity and mortality.
Methodology:
All patients admitted to JFK Medical center in Atlantis, Florida and diagnosed with COVID-19 from March 2020 to May 2020 were identified and included in this retrospective cohort. Certain demographic and clinical data were collected for each patient, including age, gender, comorbidities, complete blood count and blood chemistry values on admission. The following data was calculated: quick Sequential Organ Failure Assessment (qSOFA), the ratio of oxygen saturation to the fraction of inspired oxygen ratio (SpO2/FiO2) were calculated, presence or absence of adult respiratory distress syndrome (ARDS), and the outcome in terms of mortality. Data regarding the radiographic findings on chest X-ray (CXR) were determined to be normal, mild, moderate, or severe by a radiologist.
Patients were identified as having severe disease if they met the following criteria: Admission to the intensive care unit (ICU) during hospitalization or met criteria for ARDS.
Results:
A total of 175 patients were identified. The mean age was 62.97 years(SD 17.9years), 97 patients (55.4%) were males, 36 (20.6%) had an ICU admission during their hospitalization, 18 (10.3%) met the criteria for ARDS, 131 (74.9%) had qSOFA of 0 with only 3 (1.7%) having qSOFA of 2. The majority of CXR findings were mild 66 out of valid 155 cases (37.7%) while 19.4% read as severe infiltrate. The mean platelets count on admission was 227.71 x 109/L (SD 104 x 109/L). 43 patients (24.6%) died in the hospital.
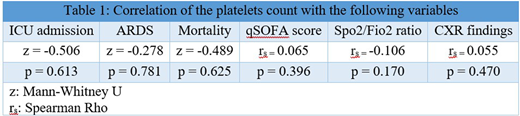
Patients with severe disease versus non-severe disease did not differ significantly in the platelet count at admission. Platelet counts were also not associated with in-hospital mortality. No significant correlation was found between the platelets count and the qSOFA scale, the SpO2/FiO2 and the CXR findings (table 2).
Conclusion:
In our retrospective Cohort study, no significant association was found between the platelet count on admission and disease severity or mortality.
Studies examining the risk factors for severe COVID-19 infection and mortality showed that thrombocytopenia is a significant risk factor.(13) Other studies showed that patients with significantly elevated platelets (> 300 x 109/L) during treatment had longer average hospitalization days.(12).
Finding practical and actionable indicators of disease severity can help clinicians guide patients with potentially worse outcomes to aggressive therapies that may lead to better outcomes when instituted earlier. More work should be done to clarify the role platelet counts can play in the prognostication of patients with COVID-19 infection.
Our Study will be followed by further investigation of the correlation between day 3 platelet count and COVID-19 severity. We are also examining the validation of a scoring system involving the platelet count among other parameters to use as a predictor for disease course and outcome.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal